
Who would have thought that there is a forgotten connection between fascia and qi? Until recently, scientists didn’t even know about fascia in the way the following article introduces them.
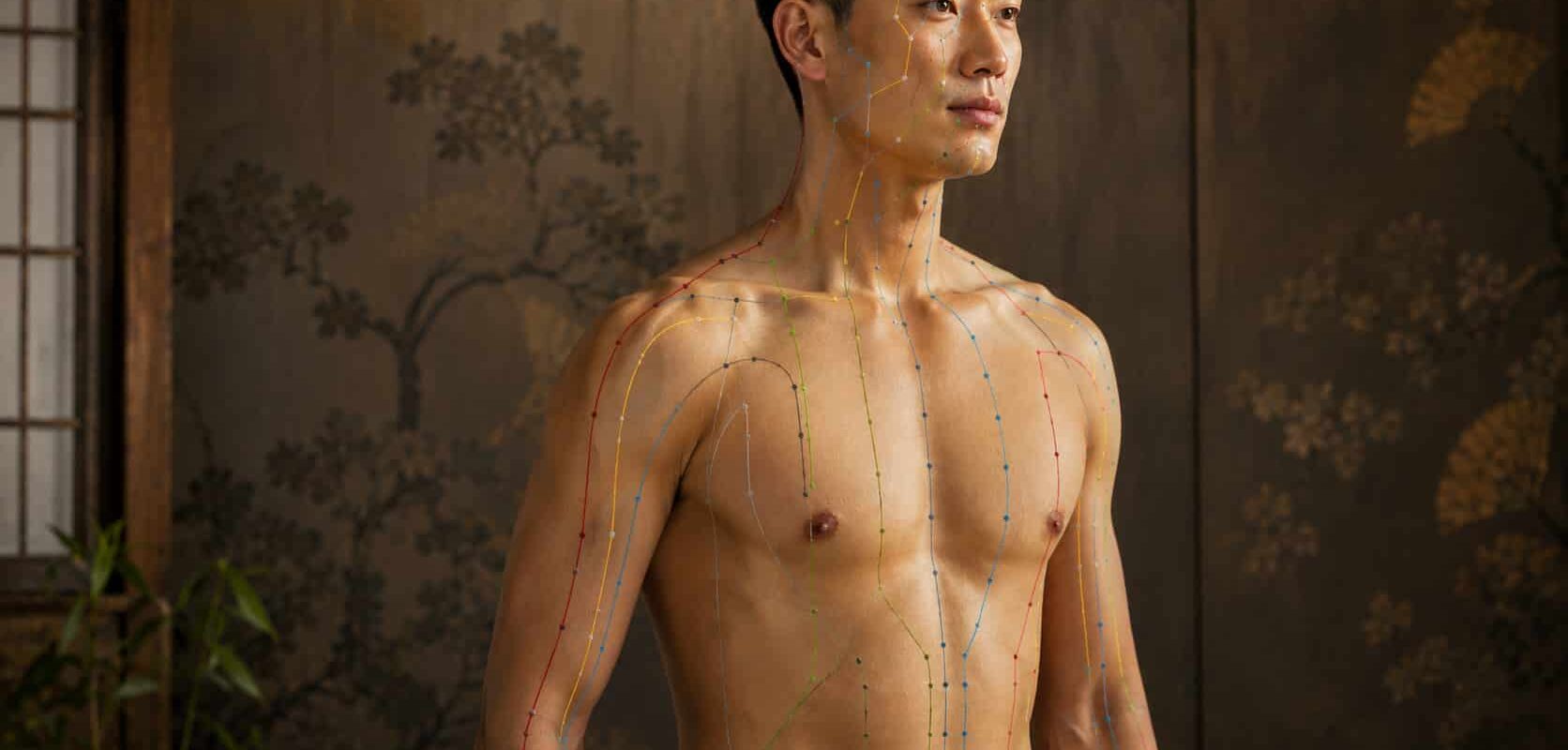
There is a moment, familiar to anyone who has been on an acupuncturist’s table, when the needle catches. Not pain. Not pressure exactly. A tug — as if the body has gripped the needle from inside. Acupuncturists have a word for this. They call it de qi: the arrival of qi. The practitioner feels the same pull through the needle, as if a fish has taken the line.
A needle goes in, and something the textbook cannot name responds
For most of the 20th century, Western medicine had two ways of dealing with this. The first was to dismiss it as suggestion. The second, more honest, was to admit that something measurable was happening — heart rate shifted, pain thresholds changed, fMRI scans lit up — but that the proposed mechanism, a flow of vital energy through invisible channels, sat outside what anatomy could verify. The needle was real. The effect was sometimes real. The map the needle was following was not.
That last sentence is no longer quite true. In the past two decades, researchers working in fascia, connective tissue, and most recently the interstitium have uncovered something that does not prove qi exists in the way the Yellow Emperor’s Inner Classic described it, but does something stranger. It shows that the meridian map — drawn by people who had never seen a cell, let alone a collagen fibril — corresponds with uncanny precision to a continuous, fluid-filled, body-spanning anatomical network that mainstream science only began to recognize in 2018.
The needle was real. The effect was sometimes real. The map the needle was following was not. That last sentence is no longer quite true.
The 80% quota, facia, and qi
In 2002, a physician-acupuncturist named Helene Langevin and her colleague Jason Yandow published a paper in The Anatomical Record that should have been more famous than it became. They took serial cross-sections of the human arm from the National Library of Medicine’s Visible Human Project and overlaid them with the classical acupuncture point and meridian maps.
They found that more than 80% of acupuncture points and the majority of meridian pathways fell along inter-muscular or intramuscular connective tissue planes — the cleavage zones where one muscle ends and another begins, the fascial gutters that anatomists use as natural surgical landmarks. Eight in 10 of the points the old Chinese physicians had marked were sitting on the fascia.
Langevin’s later work, alongside that of researchers like Robert Schleip and Carla Stecco, went further. When an acupuncture needle is rotated, the loose connective tissue immediately around it winds onto the shaft like silk onto a spindle. This is not a metaphor. It can be photographed. The wound collagen pulls on a network of fibroblasts — connective tissue cells — which respond by changing shape, signaling, and remodeling the matrix around them. The de qi grip is mechanically explicable. The needle has hooked the body’s connective fabric, and the fabric has pulled back.
Then, in March 2018, two pathologists working at NYU and Mount Sinai — Petros Benias and Neil Theise — published a paper in Scientific Reports describing something they argued anatomy had been mistranslating for over a century. Using a new live-tissue imaging tool called probe-based confocal laser endomicroscopy, they had been able to see connective tissue in its living, fluid-filled state rather than in the collapsed, dehydrated form seen on microscope slides. What they saw was not dense packing tissue. It was a body-wide lattice: open spaces filled with interstitial fluid, supported by a mesh of strong, flexible collagen bundles, running directly beneath the skin, through the fascia between muscles, around blood vessels, beneath the lining of every organ. They called it the interstitium and argued it functioned as a single, continuous, communicating system.
Eight in 10 of the points the old Chinese physicians had marked were sitting on the fascia.
The interstitium does what no other anatomical structure quite does. It runs through everything. It is the medium between the cells of an organ and the bloodstream that supplies them. It is the space through which signaling molecules, immune cells, and mechanical pressure waves actually move on their way from anywhere to anywhere else. It is, in a literal sense, the body’s connective in-between.
And it sits exactly where the meridians were said to run.
What collagen does when you stretch it, and why a needle in the wrist might be felt at the shoulder
Collagen — the structural protein that makes up most of the fascia and the scaffold of the interstitium — has a property that polymer physicists have known about for half a century, and most medical doctors still do not mention. It is piezoelectric. Stretch it, compress it, twist it, and it generates a small electrical signal. This is the same effect that lets a quartz crystal keep time in a watch.
Inside the body, this means the fascial-interstitial network is not just a passive web of fluid and fiber. It is mechanically and electrically active. A pull at one point can transmit force through the collagen matrix across surprising distances. The signal can travel as mechanical tension along the fiber, as an electrical pulse from the strain, and as fluid pressure through the interstitial spaces. None of this requires a separate nervous system or vascular system to explain it. The connective tissue itself carries the signal.

This is the structural basis for something acupuncturists have always claimed: that stimulating a point on the forearm can produce a sensation, an effect, or a release of tension somewhere else entirely. The mechanism does not need to be mystical. The body has a network whose job is precisely to transmit mechanical, chemical, and electrical information between regions that the standard organ-system view treats as separate.
Researchers in China have pushed the picture further. Dr. Hongyi Li and others have injected radioactive and fluorescent tracers into classical acupuncture points and watched them travel — not through the blood vessels or the lymphatic system, but along narrow interstitial pathways in the fascia, following routes that closely map to the classical meridian charts. Tracers injected into non-acupuncture points do not follow these lines. The channels appear to be real, at least in the sense that fluid moves through them preferentially, and the lines on the chart appear to track where fluid actually goes.
The body has a network whose job is precisely the transmission of mechanical, chemical, and electrical information between regions that the standard organ-system view treats as separate.
None of this proves that qi exists as a substance with the properties traditionally attributed to it. What it does is something more interesting. It suggests that the people who drew the original maps were tracking a real anatomical signal — interstitial fluid flow, fascial planes, mechanically reactive collagen — and naming the pattern with the vocabulary they had. They called what they could feel under their hands and observe in clinical outcomes qi. We can now describe at least part of what they were touching in the language of cell biology and biomechanics. The names are different. The thing being named appears to be largely the same.
Where the picture stops being clean
It would be a betrayal of the actual evidence to pretend the question is settled. Several caveats need to sit in the same paragraph as the discoveries above, not buried in a footnote at the end.
First, anatomical correspondence is not clinical proof. The fact that acupuncture points lie on fascial planes does not, in itself, demonstrate that stimulating those points produces specific therapeutic effects beyond placebo. Large systematic reviews of acupuncture trials consistently find weak, inconsistent, or specifically-targeted benefits — strongest for certain pain conditions and nausea, much less clear for the broader range of indications the tradition claims. The discovery of an anatomical substrate explains how a needle in the skin could plausibly produce systemic effects. It does not validate every claim ever made about what those effects are.
Second, the word qi has done a great deal of work over the past 2,500 years, and it has not always meant the same thing. Classical Chinese medical texts use qi to describe everything from breath, to the function of an organ, to a quality of climate, to a propagating signal felt during needling. To say that ‘science has discovered qi’ is to flatten a sophisticated and internally contested concept into a single biological structure. What modern research has plausibly identified is one of qi’s anatomical correlates — perhaps the most physically tangible one. The metaphysical content of the original concept is a separate question, and one that scientific anatomy is not equipped to settle in either direction.
Third, the popular claim circulating in wellness corners of the Internet — that scientists have now formally proven qi is real, and the interstitium is the meridian system — is a misreading. Theise himself has been careful in interviews to describe the parallel as suggestive, not as definitive identification. The interstitium is a real anatomical finding. The fascial substrate of acupuncture points is a real anatomical finding. The mapping between them and the meridian system is well-supported but still actively contested in the literature, with credentialed skeptics arguing that even the 80 percent correspondence may overstate the case once one accounts for how broadly meridian lines are drawn.
None of this dissolves the convergence. It sharpens what the convergence actually is. The traditional map is neither vindicated as literal truth nor dismissed as superstition. It is, on present evidence, a high-resolution observational chart of something real, made by people without instruments, that lines up with what instruments later showed.
They tracked a real anatomical signal — interstitial fluid flow, fascial planes, mechanically reactive collagen — and named the pattern with the vocabulary they had.
What this changes for someone lying on the table
If you have ever had acupuncture work for you and could not explain why, the picture above offers a structural answer that does not require you to believe in anything you cannot, in principle, measure. A needle inserted along a fascial plane, twisted to grip the local collagen matrix, sets off a mechanotransductive cascade. Fibroblasts respond. The interstitial fluid in that region is mechanically disturbed and begins to circulate differently. Local nerve endings — and there are many in the fascia — fire. Signals propagate both neurally and along the connective tissue itself. The body’s regulatory systems receive a precisely located input.
If you have had acupuncture and felt nothing, the same picture explains that too. The connective tissue varies in density, hydration, and responsiveness from person to person and from day to day. Some bodies grip the needle hard. Some barely register it. The mechanism is real, but not universally expressed.
If you are a practitioner of cultivation arts — qigong, tai chi, certain forms of meditation, Falun Dafa — the picture is in some ways even more interesting. These practices have always claimed to work directly with qi: to move it, refine it, and circulate it through the meridians and the dantian, without the intervention of a needle. The fascial-interstitial framework gives this claim a structural anchor that the older nervous-system-only models could not provide. Slow rotational movement, breath-coupled tension and release, sustained postures — these are precisely the kinds of mechanical inputs that affect collagen organization, interstitial fluid distribution, and fascial gliding. Whether or not one accepts the deeper cosmological framework of these practices, their effect on the body is no longer biologically mysterious. They are training the connective system.
What was always there
There is a habit of mind, common to both materialist and mystic, of assuming that traditional knowledge had to be either secretly correct or essentially mistaken. The fascial-interstitial story does not fit either reading. It suggests something subtler: that careful, long-running observation of the body, conducted by people without microscopes but with thousands of years of accumulated clinical attention, can identify real structures and real causal relationships, and can map them with reasonable accuracy, while describing them in a vocabulary that later science will translate but not abolish.
The meridians were not invented. They were not imagined. They were not, on present evidence, supernatural conduits of vital essence in the way some later interpretations insisted. They appear to be — at least in significant part — a clinical chart of the body’s connective tissue network, drawn from the outside in, by people who could not see the lattice but could feel where it lived and watch what happened when they touched it.
Modern anatomy, working in the opposite direction, from the cell outward, has begun to draw the same map.
The needle catches. The fabric pulls back. The chart was right.
Follow us on X, Facebook, or Pinterest